Why Revenue Cycle Management Systems Cannot Identify Legally Recoverable Revenue

Your revenue cycle management reports show collection rates meeting benchmarks. Denial management falls within acceptable ranges. Days in accounts receivable are trending down. By every standard metric, your revenue cycle is working.
Yet our analysis of surgical practices nationwide reveals something most practices don’t realize. Standard billing reports miss substantial revenue that’s legally recoverable under the No Surprises Act. Arbitration cases show that traditional RCM systems overlook recovery opportunities worth hundreds of thousands to millions each year.
The No Surprises Act changed how federal payments work for out-of-network surgical services in January 2022. Revenue cycle infrastructure still follows pre-2022 rules. These rules no longer apply to emergency services or unexpected out-of-network care at in-network facilities.
Traditional RCM Systems Miss Federal Arbitration Rights
Standard billing systems recognize three claim outcomes. Claims are either fully paid, partially paid, or denied. The No Surprises Act introduced a new issue. It involves claims where insurance pays much less than the fair market value but still marks them as closed. These systems weren’t designed to catch this problem. When payment arrives, traditional systems post it and close the file, completely missing the federal right to challenge inadequate payments through binding arbitration.
Here’s how this blind spot costs practices money. A complex surgery bills at $350,000. Insurance sends an explanation of benefits showing their Qualified Payment Amount calculation and pays $9,200. The billing team follows standard protocol by verifying the payment matches the EOB, posting it to the account, confirming the patient owes only their in-network cost-sharing, and closing the claim as successfully collected.
Every RCM metric shows success. Collection rates look good. Days in A/R improve. The billing team met their benchmarks. Yet the practice just accepted 2% of billed charges with no ability to balance bill the patient. This becomes the final reimbursement unless someone recognizes the need to pursue arbitration within the strict federal deadlines.
Traditional billing systems were built before the No Surprises Act existed. They measure whether claims got paid, not whether they got paid fairly under federal law. They track operational efficiency, not legal compliance with reimbursement standards.
The Hidden Timeline That Costs Practices Millions
The federal arbitration process runs on a different clock than your billing system tracks. And that mismatch costs practices six to seven figures annually.
When insurance underpays a claim, federal law provides exactly 30 business days from receiving that payment to initiate negotiation. Once that window closes, there are just 4 business days to file for arbitration. Miss either deadline and the right to challenge that underpayment disappears.
Meanwhile, traditional RCM systems measure aging from the date of service. They measure 30, 60, 90 and 120 days after surgery. Arbitration deadlines work differently. They run from the date insurance sent payment, not from the date you performed the surgery. Two different clocks measuring two different things. A surgery performed in January that gets paid in March starts a 30-day countdown in March, yet billing systems still track it as a 60-day old claim from January.
This timing mismatch explains staggering revenue losses across the industry. Provider testimony to government agencies reveals that insurance companies pay only their calculated QPA about 90% of the time. When providers challenge these payments, they win 77% to 85% of the time. Meaning, for every 10 cases they contest, 8 lead to higher payments.
The Legal Enforcement Gap Your Billing Company Cannot Bridge
Even winning arbitration doesn’t guarantee payment. Physician groups report substantial rates of late or incomplete payment of NSA awards. When you receive a binding payment determination, your billing company can post the expected payment and send follow-up correspondence. What they cannot do is file federal lawsuits to enforce arbitration awards.
Representing clients in arbitration proceedings and filing enforcement actions in federal court constitutes the practice of law, which falls outside what billing companies are legally permitted to provide. The Federal Arbitration Act provides mechanisms to convert arbitration awards into enforceable federal court judgments, but accessing those mechanisms requires attorneys who actively practice in federal court.
The situation is further complicated by a circuit split among federal courts. The Fifth Circuit has ruled that the NSA does not provide a private right of action for enforcing arbitration awards, meaning providers in those jurisdictions must rely on administrative enforcement through HHS. Other circuits have found an implied right to sue, creating geographic variation in enforcement options.
This creates a gap where you can successfully win a binding determination that insurance owes you substantially more, then watch that additional reimbursement disappear because the insurer won’t pay voluntarily and your billing system has no enforcement capability.
Why Legal Counsel Has Become Essential for Revenue Recovery
The practices growing revenue post-NSA have one thing in common. They added legal expertise to their revenue cycle. These practices integrate legal evaluation of payment adequacy under federal statute, implement deadline tracking that follows legal countdown clocks rather than service-date aging, and maintain federal court litigation capability for enforcement when insurers refuse to pay arbitration awards.
NSA IDR results consistently show that when providers prevail, arbitrators select payments far above the plan’s QPA, commonly several multiples, and in some specialties much higher, so a $14,200 QPA-based payment can often be moved substantially upward through a well-documented arbitration.
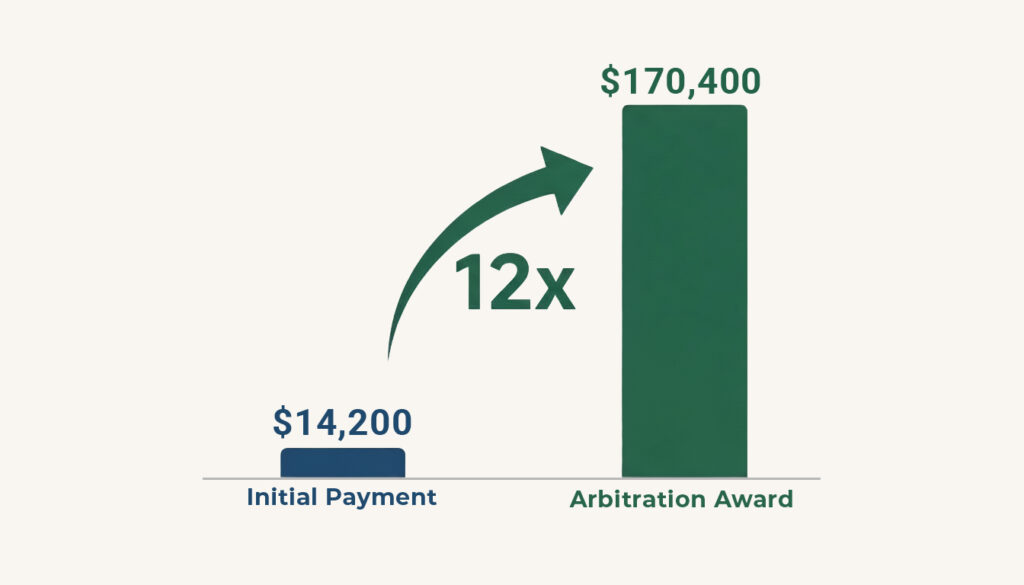
Complex neurosurgery and vascular cases have seen awards at 10-12x the initial QPA. Independent arbitrators consistently find insurance company payments inadequate when presented with proper evidence and legal arguments.
How Minevich Law Group Bridges the Gap
Minevich Law Group specializes exclusively in No Surprises Act arbitration for surgical practices nationwide. As licensed attorneys rather than billing consultants, we combine deep knowledge of medical billing with federal litigation expertise to recover what insurance companies refuse to pay.
We enforce arbitration awards through federal court when insurers won’t pay voluntarily. Our practice spans New York law with its three-year recovery window for eligible claims, New Jersey’s self-funded plan provisions, and federal NSA cases across all 50 states.
Our revenue recovery assessments show you exactly what’s recoverable. We analyze your actual claim data to identify which underpayments can still be challenged, calculate your specific recovery potential, and determine whether systematic arbitration makes financial sense for your practice.
If your practice sees payment-to-charges ratios below 30% on emergency or inadvertent out-of-network cases, you’re likely losing substantial revenue annually.
Schedule your complimentary No Surprises Act revenue recovery assessment today. Call 516-202-2196 or schedule a free consultation to discover your specific recovery potential.





